
iRehab15
Post-surgical rehabilitation platform — guides, e-consent, AI-assisted SOAP, pelvic floor protocols, daily check-ins, and clinical alerts.

Intake Compression, Not Form Consolidation: How iRehab Doctor AI Works
Most medical AI is heading toward end-to-end automation. iRehab goes the other way. Physicians don't need AI to finish their paperwork — they need it to translate two weeks of patient-reported data into a specialty-relevant summary in the two minutes before the patient sits down. Draft-Only Enforcement is the guardrail that keeps the translator honest.

First-Visit Brief: When the Patient Can't Name the Tissue
Most clinical AI demos feature the tidy post-op patient with weeks of longitudinal data. The clinic-reality majority are first visits: no history in the system, a single verbal complaint, and roughly 60–70% with no surgical need. This post is about what iRehab calls the pre-visit Brief — the short, structured summary that lands on the physician's screen before the patient sits down — and why its central design constraint is that the patient cannot answer 'is it tendon or nerve?'

From Individual Tracking to Family Recovery Coordination — The BYoAI Design Philosophy
iRehab doesn't embed AI in the app. It lets patients bring their own AI to understand their rehab progress. Why? Because the family is the unit of recovery, and AI's value isn't diagnosis — it's translation.

E-Consent for Orthopedic Research — Why Digital Consent and Hospital Branding Matter
Paper consent forms get lost, version-controlled poorly, and can't track withdrawals. How iRehab's dual-version e-consent platform and white-label theming system solve these problems for orthopedic clinical research.

When AI Learns to Write Clinical Notes — The Case for Draft-Only Enforcement
iRehab Doctor AI Phase 2 lets AI draft clinical assessments, but never auto-publish. Why we chose draft-only enforcement over full autonomy, and what it means for the future of AI in orthopedic practice.

83% of Patients Want Both — The Hybrid Future of Post-Surgical Rehabilitation
Remote monitoring after orthopedic surgery works — 92% of patients find it easy to use, and data compliance far exceeds questionnaires. But most patients don't want pure digital care. They want a hybrid model that extends their surgeon's reach into every day of recovery.

Telerehab Is No Longer 'Just As Good' — New Evidence Says It's Better
A new meta-analysis of 25 RCTs and 4,402 patients finds telerehab significantly outperforms traditional rehabilitation in pain, ROM, quadriceps strength, and cost after TKA. The evidence has shifted.

34 Exercises, 5 Phases — Inside the Evidence-Based TKA Rehabilitation Engine
Rehabilitation protocols exist in textbooks, but most patients never follow one consistently. We built a system that encodes 5 clinical phases into a daily adaptive routine — and gives surgeons a reason to trust what happens after discharge.

Recovery Loop — An Open Standard for Post-Surgical Rehabilitation
Evaluate, Prescribe, Exercise, Re-evaluate. An open rehabilitation methodology that any doctor, PT, or clinic can use for free.
Beyond Kegels — iRehab's 7 Pelvic Floor Exercises and 4 Clinical Programs
Pelvic floor training is more than 'do your Kegels.' iRehab includes 7 evidence-based pelvic floor exercises and 4 clinical programs covering pre-surgical training, post-incontinence surgery, post-prolapse repair, and non-surgical strengthening — all integrated into daily guided sessions on the patient's phone.

One in Three Women Has This Problem — Clinical Evidence and Digital Transformation in Pelvic Floor Rehabilitation
Approximately one-third of women worldwide are affected by pelvic floor dysfunction, yet fewer than 25% seek treatment. Pelvic floor muscle training (PFMT) is the first-line treatment, confirmed effective by Cochrane reviews — but long-term adherence remains poor. Mobile app-guided PFMT is changing the equation: RCTs show app groups significantly outperform traditional education in storage symptoms and quality of life improvement.

The 30-Second Daily Check-In — Designing Rehabilitation Software for 80-Year-Olds
Most health apps are designed by 30-year-olds for 30-year-olds. Post-surgical rehabilitation patients are typically 65-80. We redesigned every interaction around one constraint: if it takes more than 30 seconds, they won't do it.
Your Surgeon Knows You Skipped Today — Why Most Remote Monitoring Alerts Fail and What We Did Differently
Remote patient monitoring generates data. The hard part is turning that data into timely clinical action. Most alert systems either drown surgeons in noise or miss the signals that matter. We built iRehab's alert system around one question: which 3 patients out of 30 need attention right now?

Pain Tracking Is Pain Relief — Why Observation Itself Is an Intervention
Instead of hearing 'it still hurts' at follow-up, have patients track their pain daily. Post-surgical pain tracking works not as placebo, but through three complementary mechanisms: perceived control, anti-catastrophizing, and expectation reframing.

Beyond the Half-Truth: Patient-Mediated Continuity for Post-Discharge Health Data
When 'data follows the patient' becomes industry rhetoric, the right question isn't who owns the data — it's who makes it continuous. A Taiwan-grounded thesis after a four-platform afternoon.
User Manuals6
Role-specific operations guides for iRehab features — daily clinic use for doctors, patients, and front-desk staff.

iRehab Doctor Onboarding — From Registration to Your First Patient
Complete setup guide for iRehab: doctor registration, patient creation, exercise prescriptions, and rehab tracking. Get your first TKA patient started with home rehabilitation in 10 minutes.

iRehab Doctor PWA — Complete Feature Guide
Full guide to Doctor PWA features: patient management, assessments, prescriptions, surgical records (§A-§D), PROM auto-scheduling (19 instruments), dual-version e-consent, selfpay dashboard, Doctor AI drafts, push notifications, API tokens, and data export.

iRehab Patient App — Complete User Guide
Full guide to the iRehab Patient PWA: daily tasks, exercises, pain reports, wound photos, stamp collection, progress cards, PROM questionnaires, push notifications, and offline use.

Pre-Consult — Doctor's Operations Manual
Operations guide for iRehab's Pre-Consult feature, written for the doctor actually using it. Covers printing today's QR poster, reading the pre-consult queue, the three decision buttons, recovering lost records with the confirmation code, and six common questions. Why we built this: so the first five minutes of consultation can be about the patient, not the keyboard.

Fill This Before You See the Doctor — A Patient & Family Guide
You walked into the clinic and saw a QR Code poster, but you're not sure what to do. This guide walks you through the 2-3 minute pre-consult form, why your confirmation code matters, and what to do if scanning or filling goes wrong. You're not filling it to add paperwork — you're filling it so the doctor can spend more time with you.

Pre-Consult — Front-Desk & Assistant Operations Manual
Daily operations manual for front-desk and clinic assistant staff: pre-clinic checks, helping elderly patients and foreign caregivers, rescuing stuck forms, four doctor-collaboration scenarios, and six common questions.
Orthopedic Innovation14
Implants, sensors, outcome measurement, and the future of orthopedic practice — from WingHeal to CMS TEAM.

Why Your Surgeon Should Be Tracking PROM After Joint Replacement — And Why Most Don't
Only 25% of joint replacement patients complete functional outcome tracking at one year. CMS now mandates 50% collection by 2028 or face payment penalties. PROM isn't just a questionnaire — it's the compass that shows both surgeon and patient the full picture of recovery.

The Complete Guide to Rehab After Knee Replacement — Every Milestone from OR to Daily Life
Enhanced recovery protocols now get TKA patients home in 1-3 days instead of a week. But the real challenge starts at discharge: 12 weeks of rehabilitation that determine what your knee can do for the rest of your life. This guide integrates the latest 2025 clinical evidence to walk you through every milestone.

Remote Monitoring After Knee Replacement: AAOS 2026 Confirms It Works — Even for Older Patients
New data from AAOS 2026 validates remote therapeutic monitoring after TKA in geriatric populations: no increase in complications, lower costs, and successful deployment at scale. Here's what it means for orthopedic practice.

How AI Is Changing Orthopedic Care — A 2026 Field Report
In 2025, the FDA cleared a record 295 AI medical devices. Fracture detection hits 98% accuracy. ML models predict TKA dissatisfaction before surgery (AUC 0.888). But the real AI battleground in orthopedics isn't the operating room — it's the 90 days after discharge.

Same-Day Joint Replacement Is Here — Who's Watching Your Recovery?
Over 60% of total knee replacements in the US are now same-day discharge — up to 80-99% at select ASCs. CMS is phasing out the inpatient-only list by 2029. Danish fast-track centers hit 94%. Hospital stays dropped from 5 days to near zero — but who fills the 90-day monitoring gap?

CMS TEAM Model: What 741 Hospitals Must Do Now — The Mandatory Bundled Payment That Changes Orthopedic Practice
January 2026: CMS launched TEAM — the first mandatory bundled payment model covering joint replacement, spinal fusion, and CABG at 741 hospitals. PROM collection is required, 30-day episodes are tracked, and there's zero infrastructure funding. Here's what orthopedic practices need to do now.

RTM Billing Guide: The $77-Per-Patient Monthly Opportunity You're Missing
New 2026 CMS RTM codes slash the monitoring threshold from 16 days to just 2. CPT 98985 pays $51 for MSK monitoring, plus $26 for treatment management. Here's exactly how orthopedic practices can bill for post-TKA remote monitoring.

TEAM Model Q1 Reality Check: What 741 Hospitals Are Learning the Hard Way
Three months into CMS TEAM, 741 hospitals face patient attribution gaps, fuzzy PCP referral mandates, and rural care coordination failures. These implementation pain points reveal exactly where post-surgical monitoring platforms fit.

The Digital MSK Consolidation: Sword Buys Kaia, Hinge IPOs — Where Is the Real Moat?
Sword Health acquires Kaia Health for $285M. Hinge Health IPOs at $3B with $588M revenue. The digital musculoskeletal market enters its consolidation phase. But when exercise libraries become commodities, what actually constitutes a defensible position?

Why Bones Need Wings — The Design Philosophy Behind WingHeal
Rotator cuff repair faces a dilemma: insufficient strength leads to re-tear, and excessive immune response causes rejection. WingHeal combines a PEEK structural augment with low-immunogenic collagen scaffold, showing +71.8% biomechanical stiffness and fibrocartilage formation at 4 weeks in animal studies.
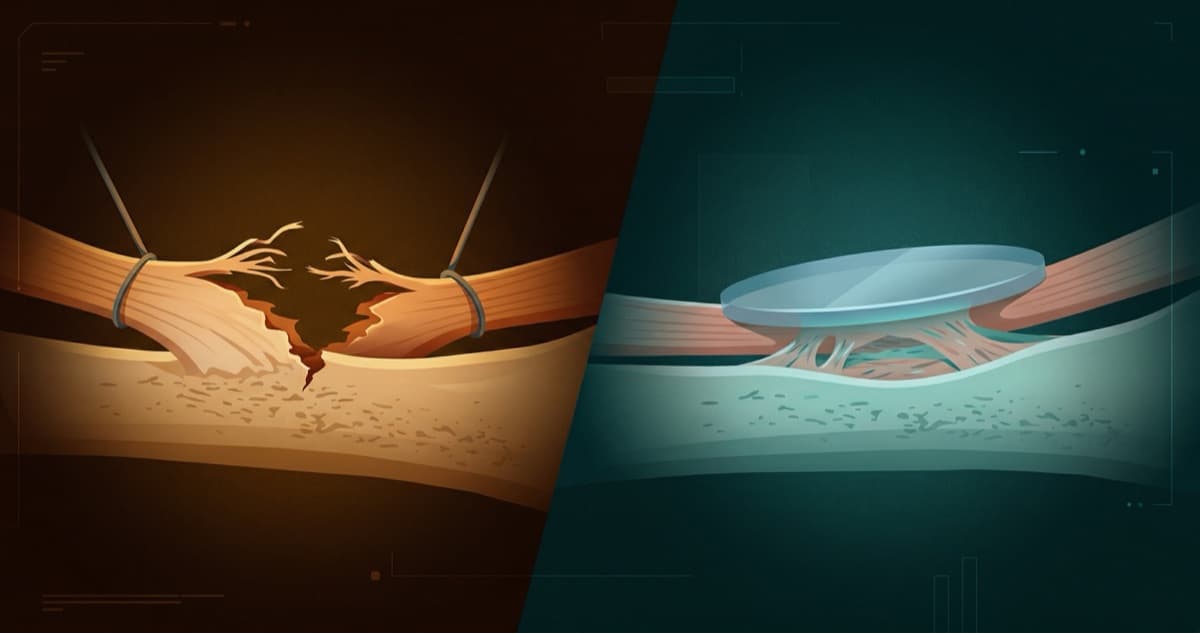
The First Principle Everyone Agreed On — That Nobody Followed
Every orthopedic surgeon agrees: even pressure distribution improves tendon-to-bone healing. Yet a decade of fear after SIS patch failures kept anyone from building the obvious solution. WingHeal starts from first principles.

The Sentinel Inside the Bone — How Implantable Sensors Are Changing Post-Surgical Monitoring
Traditional post-surgical monitoring relies on imaging and patient-reported outcomes. Discovery R uses a battery-free LC resonant sensor to measure forces at the implant site in real time, detecting 'impending failure zones' during movement — not after structural damage has already occurred.

The Race Inside the Bone — 2026 Implantable Sensor Landscape
AO Foundation's fracture monitor enters first-in-human trials. Penderia earns FDA Breakthrough Device Designation. CardioMEMS proves passive LC sensors work at scale. The real competition isn't which sensor is best — it's who can turn sensor data into clinical decisions.

When AI Makes Software Free — Implantable Sensors, Thick Software, and the Real Moat
GPT lets anyone build a SaaS in a weekend. When software is no longer scarce, where does value migrate? To data — but not just any data. Data that others cannot replicate. Tissue force data from implantable sensors is that kind of data. This article explains why thin software dies, thick software thrives, and where sensors fit in the game.
xGrid Platform1
Field station operations, offline-first architecture, and disaster resilience — from power-on to daily management.
Resilient Systems7
Design philosophy, system architecture, clinical workflows, and battlefield medicine — why we build differently.

When the Wall Is Breached — Designing Medical Systems with Safety-II
Safety-I builds walls against failure. Safety-II asks how people succeed despite failure. In disaster medicine, the difference determines whether a forced evacuation loses patients or saves them.

The Walkaway Test — Designing Software That Outlives Its Creators
What happens when the development team disappears? We formalized the software industry's 'bus factor' problem into five rigorous acceptance criteria — and built a medical system that passes all of them.

Offline-First Is Not a Fallback — How xGrid Runs Without the Internet
Most medical systems treat offline mode as degradation. xGrid treats it as the default. When your deployment site has no cell towers, no routers, and no IT staff, every design decision starts from zero connectivity.

Unplug and Go — Hub-Spoke Designed for Disconnection
Traditional Hub-Spoke carries one fatal assumption: the Hub is always online. But in a disaster zone, when the Hub goes down, patients cannot wait. xGrid designs for disconnection as the normal state — every node is a complete system, and any one of them can take over.

Triage Is Not Classification — It's the First Resource Allocation Decision
Triage is not about sorting patients into color categories. It is about deciding who gets what resources, when, and at whose expense. In xGrid, the color you assign determines the bed, the drugs, and the surgery slot.

ISBAR Is More Than a Handoff Format — What Happens When Oral Tradition Meets Structured Data
Clinical handoffs have been oral for decades. ISBAR gives them structure. But the real value is not the structure itself — it is what becomes possible when handoff data is searchable, verifiable, and replayable.

Burn Rate & Approvals — Resource Intelligence and Collective Accountability in Battlefield Medicine
How long until we run out of O-negative blood? Who authorized the amputation? xGrid's burn rate engine calculates hours-to-depletion in real time, while the multi-signature approval system ensures irreversible decisions are never made alone.
AI Work Discipline1
Disciplines, review patterns, and governance lenses that keep AI-assisted knowledge work from collapsing under its own output.
